
Children face all kinds of risks after the death of parents
The problems expounded above persist after the parents’ death. Added to the emotional and material vulnerability already described is the destruction of the family and psychosocial distress that afflicts any type of orphan. The question arises: Are AIDS orphans even more vulnerable than other orphans?
Economic Problems
After the death of parents, factors such as loss of household incomes, treatment costs for illnesses linked to HIV and then funeral expenses often leave orphaned children impoverished. A study carried out in four provinces of South Africa established that households that have lost one of their members to HIV/AIDS have devoted, on average, one third of their annual income to funerals during the previous12 months Steinberg, Johnson et al., 2002.
Additionally, as reported above, orphans are easily dispossessed of their inheritance when the parent dies, which increases the economic problems already present.
According to the 1999 Demographic and Health Survey carried out in the United Republic of Tanzania, dependency ratios are higher for households caring for orphans than for other households with children. Therefore the problem of orphans should be considered in a context of poverty National Bureau of Statistics and Inc., 2000.
The situations vary according to the identity and gender of the person responsible for the orphans and whether residing in a rural or urban setting. Female-headed households that include orphans in rural areas record the highest dependency ratio Monasch and Boerma, 2004.
Financial problems determine all other problems Memain-Yenou, Coulibaly-Traore et al., 1998. Therefore, reduced economic capacity for households that include orphans means difficulties in satisfying the children’s and orphan’s basic needs, including education, food security, health, clothing, etc. and promotes child labour.
Child labour
A study carried out in Zambia focused on the growing number of children who work related to the HIV epidemic, noting an increase from 23% to 30%. Mushingeh, Mkandawire et al., 2002
Studies and surveys on child labour have proven indispensable to assess and measure this phenomenon among orphaned children more carefully.
Concerning this, “rapid assessments carried out by the International Labour Organization to investigate the situation of working children found that orphaned children are much more likely than non-orphans to be working in commercial agriculture, domestic service, commercial sex and as street vendors” Semkiwa, 2003.
Moreover, these rapid assessments have provided proof that most working children were orphans who had lost their parents due to HIV.
“The assessments indicate strong links between HIV/AIDS, orphanhood and the worst forms of child labour” UNICEF, UNAIDS et al., 2004.
Difficulties in accessing education
Most researchers agree that HIV/AIDS poses serious consequences on education due to the reduced economic capacity of foster families who struggle to ensure their orphans’ education.
Orphans’ education is not a priority due to the lack of financial means, causing a drop in school attendance and often high drop-out rates Kelly, 1999. Difficulties in accessing education occur before the death of a parent. Numerous children whose parents are infected by the disease drop out of school because they must care for their parents. They are often required to work and abandon their educations or are excluded from the school system mostly because of their absenteeism Yaro and Dougnon Denis, 2003.
These problems persist after a parent’s death. The children who have become orphans lose emotional and financial support. They must often work to cover essential needs for themselves and their younger siblings if they are responsible for them.
“This often results in dropping out of school, given that work and education are a dichotomy” Yaro and Dougnon Denis, 2003. Yaro et al., show that nearly eight out of ten orphans in Burkina Faso have dropped out of school. For example, one said that he was always at the top of his class for the first five years at primary school. When he lost his father and then his mother several months after, his grades dropped below average. He explained it by the fact that he was starving when he left for school and when he returned home he had to do domestic chores before resting. Soon, he was unable to handle the excessive workload outside of school and had to quit school in spite of himself Yaro and Dougnon Denis, 2003.
According to J. Wakam, the situation for orphans is still deteriorating with the economic crisis; the household standard of living has become more decisive for education than in times of prosperity Wakam, 2002. Another study conducted in Kenya shows that education is the main problem for guardians of orphans. This is due to the lack of resources in households with orphans, which mainly function on a subsistence economy Nyambedha, Wandibba et al., 2001. In addition, Nalugoda et al. also show a low enrollment rate in the district of Rakai in Uganda for children who have lost a parent Nalugoda, 1997.
Likewise, UNICEF underlines the important number of orphans in sub-Saharan Africa who do not finish school UNICEF and UNAIDS, 1999. Moreover, UNESCO has implemented special programmes on education planning in the HIV context Kelly, 1999. In response to the mounting problem, the governments of Malawi, Uganda UNICEF and UNAIDS, 1999, and Kenya Republic of Kenya, 2001 have enacted measures to abolish school fees for orphaned children.
Other studies confirm that orphans suffer more vulnerability than non-orphans in terms of education in the context of HIV/AIDS Grassly and Timaeus, 2003, Nampanya-Serpell, 2001, Foster, 2000, Foster and Williamson, 2000, Urassa, Walraven et al., 1997, Muller and Abbas, 1990.
Poverty is not the only cause for an orphan’s absenteeism. The determining factor is the nature of the family relationship between the orphan and the adult who makes decisions in the family; the closer they are, the more likely the child will go school. Thus, children living in households headed by someone other than their parents are more disadvantaged than those living with their parents, and children who have no kinship with the head of household have even more difficulties Case, Paxson et al., 2004.
Therefore, it is essential to take into account the various family contexts for orphans (for example, whether they have lost one or two parents), their living situation (for example, urban or rural), and gender to define problems as well as solutions.
Moreover, according to Y. Yaro et al., “when an orphan has lost one of his or her two parents, he or she has only 50% chance to access to school and only 10% when it is both parents” Yaro and Dougnon Denis, 2003.
Additionally, discrimination linked to the loss of a parent from AIDS holds up children from pursuing their education. Furthermore, according to Y. Yaro et al., “in Burkina, during focus groups with orphaned children, they pointed out that their best friends shunned them after their parents’ deaths. Although the orphans had tried to connect with their old friends, they continually avoided them, even refusing to play with them because, according to them, it was possible that they would contract the disease of their deceased parents. Quite often these discriminatory attitudes, held through the students’ lack of knowledge, are maintained by the parents themselves.” Yaro and Dougnon Denis, 2003
Not only is the number of children who do not attend school rising at an alarming rate (for example, in Zambia, 30% to 40% of orphans do not go to school), but teachers are also hit hard by the pandemic. More than one thousand teachers die of AIDS each year in Zambia, faster than it is possible to train new ones Kelly, 1999.
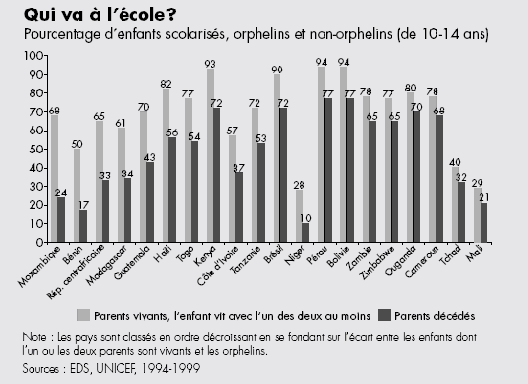
The graph below confirms these findings:
Figure 7 : Who goes to school? Percentage of children attending schools, orphans and non-orphans.
However, some studies show different results:
Monasch and Boerma calculated the different school attendance rates between orphans and non-orphans across 31 sub-Saharan African countries. School attendance rates for orphans (ages 10 – 14 years) are expressed using a ratio that compares the proportion of orphans to non-orphans in the same age group who attend school. If there is no difference between the orphans’ and the non-orphans’ school attendance rates, the ratio equals one. Therefore they observed that in 30 of the 31 countries studied, this ratio is not significantly different from one and that there were no noticeable differences in access to education between orphans and non-orphans. However, the gap for school attendance between orphans and non-orphans is further marked in countries where school attendance rates are low. Furthermore, double orphans appear to be more disadvantaged than single orphans Monasch and Boerma, 2004.
Other studies, especially those conducted in Uganda and Tanzania, have confirmed these results Kamali, Seeley et al., 1996, Urassa, Ng'weshemi et al., 1997. Conversely, in Sierra Leone, Mali, and Nigeria Bledsoe, Ewbank et al., 1988, Oni, 1995, Castle, 1995 no difference was observed between girl and boy orphans regarding their education, contrary to a priori assumptions.
Difficulties accessing health
Assessing the impact of orphanhood on health in the HIV/AIDS context rests on three indicators: malnutrition, stunted growth, and infant mortality. The studies present discrepancies in terms of the estimated impact of parent deaths on these indicators.
Some studies concur that in families affected by HIV/AIDS “food consumption can drop by more than 40 per cent, putting children at higher risk of malnutrition and stunted growth” UNICEF and UNAIDS, 1999.
In Tanzania, studies show that the death of the father, mother, and other adult members in the household cause stunted growth among affected children. This result is also confirmed within households that are not impoverished. Thus, poverty is not an explaining factor for stunted growth among orphans; by contrast, in impoverished households, the status of orphan exacerbates stunted growth Ainsworth and Semali, 2000.
In Zambia, average calorie consumption has decreased over 20 years from 2273 to 1934 calories per day. According to the UNCTAD (United Nations Conference on Trade and Development) this drop is chiefly attributable to AIDS since HIV/AIDS has reduced activity, production, and consumption rates Cessou, 2005.
In Zimbabwe, a 2003 nutrition survey weighed and measured 42 000 children of whom 1760 were orphans. This study showed that orphans suffer malnutrition at a higher proportion than non-orphans Ministry of health and child welfare, 2003.
In Uganda, a study showed that the death of mothers causes a rise in infant mortality, even among HIV-negative children Nakiyingi, Bracher et al., 2003.
In a study on relationships between the adopted child and infant mortality in Sierra Leone, Bledsoe and Brandon (1992) show that mortality risks are higher among adopted children than among biological children, resulting from discrimination and food deprivation Bledsoe and Brandon, 1992. Similar results were found in West Africa Bledsoe, 1990, Bledsoe, Ewbank et al., 1988, Oni, 1995. This excess death rate among orphan children may be linked to mother-to-child HIV transmission; “approximately 20% to 40% of these orphans are born HIV-positive and rapidly progress to AIDS, often dying before their fifth birthday” Delcroix and Guillaume, 1997.
This can also result in orphans receiving differential treatment compared to other children, depending on the type of relationship that exists between the adoptive and biological parents. This reflects family instability in the foster home Bledsoe, 1990 or a more or less voluntary caretaking for this child Madhavan, 2004. Castle (1996) has shown in Mali that children who were voluntarily taken in did not suffer from malnutrition, while children who were involuntarily adopted were undernourished Castle, 1996.
However, other studies lean toward opposite conclusions:
Monasch and Boerma observed little impact on nutritional status for orphaned children in a study carried out in 40 sub-Saharan African countries Monasch and Boerma, 2004. In Zambia, Namposya Nampanya-Serpell show that nutritional impact from parental loss mainly depends on the children’s age (the youngest were exposed to greater risks than older children), but also the on the foster home’s socio-economic status Nampanya-Serpell, 2001.
In a study conducted in Tanzania, Urassa et al., observed that the mortality rate for orphans and foster children is not higher than that of other children Urassa, Ng'weshemi et al., 1997. Foster arrived at the same conclusion through a study conducted in Zimbabwe Foster, 2000, as did Kamali et al., in Uganda Kamali, Seeley et al., 1996.
Psychosocial impact and stigmatisation due to HIV/AIDS
A child’s trauma and fear are universal feelings caused by the disease and the loss of a parent. HIV infection and the disease’s debilitating effects can cause psychosocial distress among children, characterised by fear of the future and of parental death. This fear is reinforced by the culture of silence and denial of reality within the family, denial that is specific to HIV/AIDS, which is considered a “taboo” disease in many societies Landis, 2002.
The specificity of HIV/AIDS is that it affects and distinguishes children from a psychosocial point of view before the death of parents.
A 16-year old South African girl living with a family affected by HIV/AIDS claims: “They treat you badly. You don’t feel like walking in the street, they give you names. They whisper when you pass. They take it that when one person in the house is sick, all of you in that house are sick” Save the Children, 2001.
Indeed, HIV/AIDS is perceived as a disease that is judged as “immoral” and “dirty” Sontag, 1989, a “shameful disease” Dozon and Guillaume, 1994 that is harshly stigmatised in African societies. Among the Mossi in Burkina Faso, “the AIDS sufferer “ruins” the family name and dishonours it. (…) This fear drives some families to hide their sick relative” Taverne, 1997.
Lack of knowledge about HIV/AIDS and its transmission increases fears and prejudices about the rest of the family members. The whole family is suspected to be infected by the disease. After their parents’ death, AIDS orphans suffer intense discrimination based on the unjustified fear of contamination. According to a study conducted in Uganda, some family members suspect that the orphans are HIV-positive and hence fear for themselves and their children; even if they are taken in, the orphans remain isolated even within the family Ntozi and Mukiza-Gapere, 1995. Stigmatisation is one of the reasons why families hesitate or refuse to take in orphans whose parents have died of AIDS Seeley, Kajura et al., 1993. The notion of “AIDS orphans” contributes to this stigmatisation, explaining why the term should be used with caution UNICEF, UNAIDS et al., 2004.
HIV/AIDS has not only created orphans from parents, but also “orphans from society;” although traditionally, the concept of social orphan does not exist within communities. Therefore, HIV/AIDS has profoundly transformed the fundamentals of support and its obligations Taverne, 1997.
Orphans can be treated as “second-class members” of the foster family. They are put at a disadvantage when supplies are distributed or work is divided up, and they suffer from lack of affection. The foster family favours their biological children who receive preferential treatment Nyambedha, Wandibba et al., 2001.
A study carried out in Zambia indicates that orphaned children feel different from other children mainly due to their lack of education Family Health International and USAID/Zambia, 2002. These children’s well-being is hindered; most of them have very little hope or optimism about their future, as shown in a study conducted in Uganda (Figure 9).
In addition to the suffering endured because of this discrimination, orphans suffer from separation from their siblings once they have been placed in the kinship network Nampanya-Serpell, 1998.
In a study in Uganda, orphans (aged more than 13 yeas) when asked explicitly about how they felt about being apart from their siblings, older orphans (n=64) report feeling sad (43.8 percent) and feeling isolated (17.2 percent)Gilborn, Nyonyintono et al., 2001. Other studies confirm the harmful effects from separating siblings Nampanya-Serpell, 2001; McKerrow, 1996. Breaking up siblings has seen a high prevalence in countries such as Zambia and Congo-Brazzaville. In Zambia, the previously cited study shows that 56% of orphaned children who are taken in were separated from their siblings. Furthermore, there is an extremely low frequency of reunion between siblings who were once separated Family Health International and USAID/Zambia, 2002.
In Congo, a study carried out on orphaned children in Brazzaville found that 63% of them were separated from their siblings, causing serious psychological difficulties for these children Mboussou, Mkaya Julien et al., 2002. (Figure 8)
Finally, the most recent studies emphasise how important it is for children’s psychological health to avoid separating siblings when placing orphans Ruiz-Casares, 2005.
Figure 8 : Orphans are likely to be separated from their siblings.
Four districts in Zambia, 2001
Figure 9 : Orphans are less optimistic about their future.
Psychological effects of orphanhood in Rakai, Uganda, 1997.
All of the previously stated problems are obviously exacerbated when orphans do not receive care. Their vulnerability increases when they are left on their own with neither parental protection nor parental substitutes.
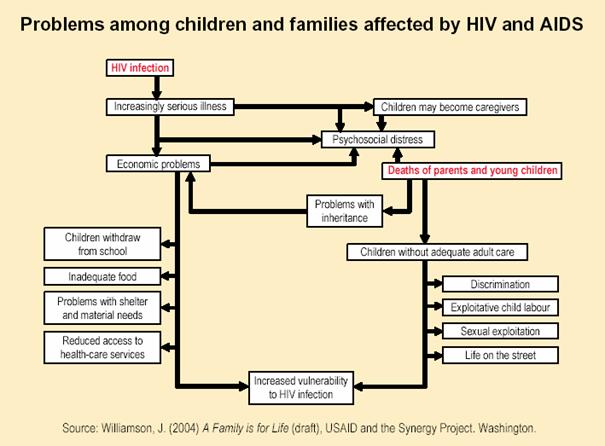
Figure 10 : Problems among children and families affected by HIV AIDS
^ Top
| Acknowledgments |